A generation lost: Fear and self-loathing in HIV-ridden Larkana
As the number of HIV cases rises to over 650, health authorities' efforts to control the situation seem too little

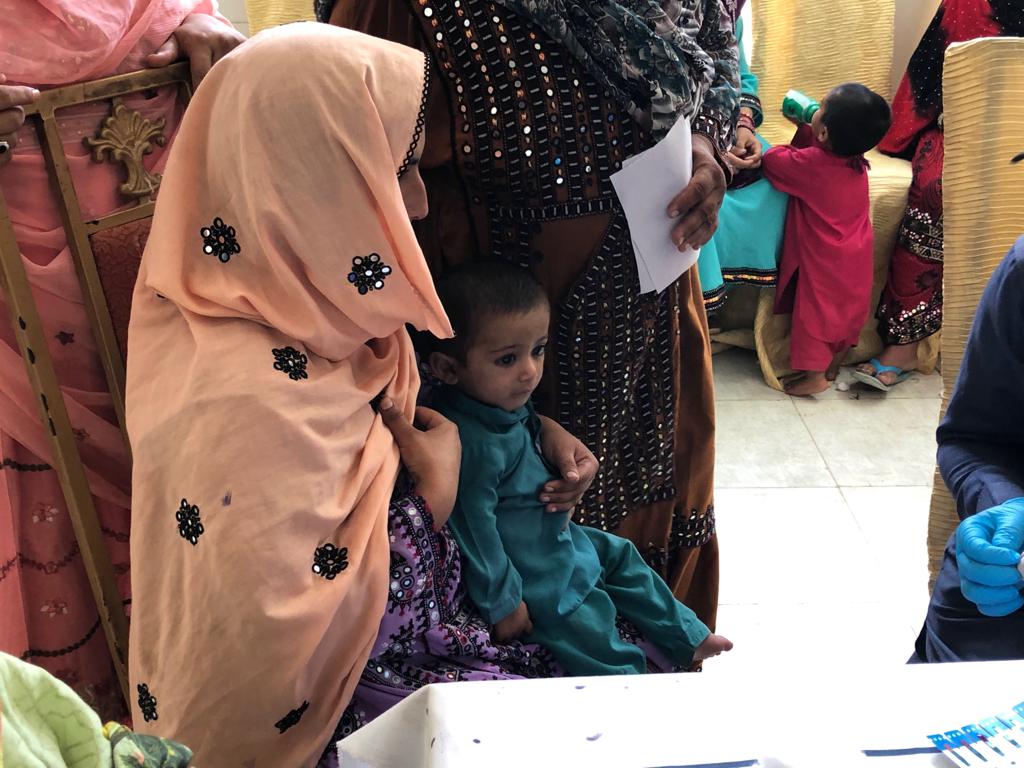
Long lines: Women and children waited for several hours at Rato Dero Taluka Hospital to be allowed inside the facility, where they would be tested for HIV. As thousands made their way to the screening camps, authorities found it difficult to manage the influx. Photo: Express
It didn’t make much sense - weren’t doctors supposed to heal? Well, not this one apparently. Dr Muzaffar Ghangaro, who has gained notoriety for infecting hundreds of children with the Human Immunodeficiency Virus (HIV), is currently in judicial custody after it emerged that he was the man behind the outbreak of the disease. The damage has, however, been done and hundreds of children will spend the remainder of their lives enduring the consequences.
Since reports of the outbreak surfaced, thousands of residents of Rato Dero — a small town with a population of 0.33 million according to the latest census, located 30 kilometres to the north of Larkana — have gotten themselves screened at one of the six screening camps set up by the provincial health department, in collaboration with other private and government agencies. At least 681 were confirmed positive for HIV out of the 23,174 people tested by Saturday [May 25], of whom 558 were children.

“What surprised us is that 90% of the children who tested positive had been treated by Dr Ghangaro at some point,” remarked Nazeer Ahmed Soomro, the focal person of the National Aids Control Programme (NACP) posted at the main screening camp set up at the Rato Dero Taluka Hospital. “None of their parents tested positive for the virus which could only mean they were infected via a transfusion or with the prick of a needle,” he added.
“We want him to be hanged,” interjected one woman, S*. She had come to the camp from Khan Muhammad Rind village with her five-year-old son, who had just tested positive in the first two stages of the screening. He will undergo one additional test at the Larkana Civil Hospital, which would decide the course of his life.
The screening
With the world’s attention turning towards the outbreak that has suddenly taken the sleepy town of Rato Dero by storm, all government agencies are working in overdrive to control the situation.
Lady health workers are visiting each village to advise residents to get themselves and their children tested for the virus. The Peoples Primary Healthcare Initiative (PPHI), Integrated Health Services (IHS) - both public-private ventures, the Sindh Aids Control Programme (SACP) and its federal counterpart, United Nations Children’s Fund (UNICEF) and the World Health Organisation (WHO) have all teamed up to figure out how many people have actually been affected.

Residents are directed to visit one of the six screening camps set up by the agencies.
“We have been testing around 150 to 200 people a day,” said PPHI’s Dr Sabeen Abbasi, who was filling out forms with the patients’ particulars as they went through the first round of testing at the Rato Dero Taluka Hospital. There are at least four other rooms dedicated for the initial round of testing.
“When a patient comes in, we register their details and then prick their finger to obtain a blot of blood to test with the strip,” she explained. The tester, in this case, is the Alere strip that is used to detect the p24 antigen and HIV-1 antibodies.

If there is a reaction, the patient is sent for secondary screening, which is in another room at the same facility. This time, the patient is tested with SD Bioline, which also tests for the presence of antibodies specific to HIV.
Both testing materials have been recommended by the WHO, which then provides it to the SACP. “There is a 95% chance that the patients coming through from the initial testing will test positive in the secondary screening,” said the NACP’s Soomro.
If the patient is unfortunate enough to test positive in that too, they will be referred to the Larkana Civil Hospital, where they will be screened a third time, using the Uni-Gold test. This third step is designed to not only test the patient for the presence of the virus but also quantify it to help the doctors decide the course of treatment.
The treatment
“If all three tests return positive, the patient is immediately started on the antiretroviral therapy (ART) unless they are suffering from tuberculosis,” said Soomro. “If the latter is the case, they are given medication for TB for a month before being started on the ART,” he added. In any case, the patient has to take the medication for the remainder of their lives, else the virus could progress into Acquired Immunodeficiency Syndrome (AIDS), which is where it becomes fatal. This is when the count of CD4 cells - a type of white blood cells that are part of the human immune system - depletes below 200.
“In all the cases to have come out of Rato Dero so far, thankfully no patient has a low CD4 count,” said Dr Shah Muhammad Sheikh, the focal person of the SACP, posted at the Rato Dero Taluka Hospital. What this also means is that the majority of the patients have been infected quite recently as the virus hasn’t progressed to its next stage yet.
Unfortunately, he can’t be too sure of the numbers, simply because not every child who tested positive at the taluka hospital was taken to the newly established HIV/AIDS centre at the Children’s Hospital in Larkana. In fact, of the 535 children who had tested positive by Thursday (May 23), only 362 had registered with the centre. Of these, 147 had been started on the ART medication, said Dr Irfan Sheikh, the in-charge at the centre.

Dr Sheikh, who has been looking after the centre since May 16 - six days after it was set up - checks each patient physically, besides looking at their test results.
Seated beside him is Dr Zulfiqar Ali Rahijo, a consultant psychiatrist, who counsels the patient’s family on how to deal with the ailment. “These children are too young to understand what is happening, but we must make sure the parents appreciate the severity of the situation,” said Rahijo.
For adults, who are treated at the HIV/AIDS centre operational at the Larkana Civil Hospital since 2007, the process is fairly similar. If a patient tests positive, they are started on the ART, while the patient and their family are counseled by a psychiatrist.
Naseer Ahmed, the psychiatrist posted at the hospital since 2012, told The Express Tribune that each counseling session lasts 25 to 30 minutes and includes discussions with the patient’s family too. “We also encourage patients to interact with each other as a sort of group therapy,” said Ahmed. “If one patient sees another getting better with medication, they too are motivated to follow the same course and take their medication regularly.”
Dr Hola Ram, the in-charge of the centre, believes most adult patients have been infected via sexual transmission. He bases the assertion on the patients receiving therapy at the centre. He admits, however, that the reuse of syringes presents a significant challenge - one that needs to be urgently addressed by the relevant authorities.

The scare
This realisation may, however, be a little too late for the parents whose children will have to suffer the consequences of some doctor’s actions for the rest of their lives. It has been 25 days since the screening camps were set up; five days after a local doctor pointed out that something was remiss.
That doctor would be Imran Akbar Arbani, who has a private practice in Rato Dero Town, minutes away from the Taluka Hospital. “I unearthed the outbreak,” he exclaimed proudly. Behind his shoulder stands a frame, proclaiming him to hold the honour of removing the largest kidney stone in the world. Somehow, that story finds its way into the conversation too.
But Arbani means business when he says he broke the news. “It all started in the end of February with Iman Fatima, a 16-month-old girl, who was brought to my clinic with high-grade fever and pneumonia,” he recalls. The child had been taken to several doctors, but no one could figure out why her fever persisted. “The minute I saw her, I suspected it was HIV,” he said. What surprised Dr Arbani was that none of the other doctors had even thought of it. “This shows you what the SACP has been doing for the past 24 years of its existence,” he spat.
The child was referred to the Aga Khan University Hospital in Karachi, where she tested positive for HIV and was placed under the care of Dr Fatima Mir. She was able to regain her strength and returned home after a month.
Over the next couple of weeks, Dr Arbani noticed at least 15 other patients who had the same symptoms. He referred them all for HIV screening. All came back positive. “Each time a child was brought to me, I would automatically send them for screening.” In all, 85 of Dr Arbani’s patients tested positive for the virus.
“They [SACP] refused to believe me and tried to play it down, but now they know what they’re dealing with,” he said with a smile. Over 650 people have tested positive since the screening camps were set up. For Dr Arbani, however, this is just the tip of the iceberg. “You know, the one that caused the Titanic to sink,” he joked. The number could rise well into the thousands if the SACP did the screening properly.
The numbers
Dr Arbani’s prediction may seem far-fetched but the general practitioners in the healthcare sector in the province make his assertion quite believable. The Sindh Health Care Commission, which is supposed to register and monitor healthcare facilities has largely been non-functional until very recently.
Its officials blame lack of resources each time they are asked about their performance. In the meantime, quacks rule the roost in most small towns and villages, offering cheaper, hassle-free alternatives to primary healthcare units.
The NACP’s Soomro blames people equally for this. “People prefer to go to these private clinics even when they can easily go to the government-run facility.” Soomro attributes this to the negative perception about government facilities in general. In Dr Ghangaro’s case in particular, the added charm was that he would charge only Rs35 as consultancy fee. “He was the cheapest option available for miles around,” said Soomro.

Lack of awareness
While quacks and bad medical practices at private clinics are being blamed for the current epidemic, Larkana district is no stranger to such an outbreak. In October 2016, an HIV outbreak was reported among over 50 patients of renal dialysis at the Chandka Medical College Hospital in Larkana. The patients had contracted the virus through the transfusion machines that were part of the dialysis procedure. The tertiary hospital, run by the provincial government, did not screen the patients coming in for dialysis, even though the hospital had its own HIV unit.
At the time, the case did raise some noise, but interest soon died out and the practices continued.
“What has the SACP been doing all this time?” questioned Dr Arbani. It took another epidemic to jolt the programme’s officials into action. “The SACP believed HIV was only restricted to ‘high-risk’ communities,” he said, referring to sex workers and drug abusers. All their campaigns, if any, were limited to raising awareness among these two groups. What they missed out was the general population that was also at high risk due to bad medical practices, particularly the reuse of syringes, which is what has been identified in Dr Ghangaro’s case.
“The reuse of syringes is rampant in the region,” admits NACP’s Soomro. Again, the problem was believed to be limited to drug abusers, who used syringes thrown away by medical practitioners to inject the narcotic substances. This time, however, quacks are to blame.
There is a simple way to stop the reuse of syringes - use auto-lock syringes instead. In fact, the Sindh Assembly passed a law to this effect as far back as 2011. Summarily, the Sindh Regulation and Control of Disposable Syringe Bill, 2010, stated that “no person shall manufacture, sell or use disposable syringes other that auto lock, auto destruct or auto break for injection, drawing of blood and other purposes.”
Yet again, there has been no implementation. Walk into any store selling surgical equipment in Larkana’s Shahi Bazaar and you will be hard-pressed to find auto-lock syringes for sale.

“They just aren’t viable,” Muhammad Ali, a surgical equipment wholesaler in Larkana told The Express Tribune. “Each auto-lock syringe costs Rs30, while the regular one costs Rs6,” he explained. The point he is trying to make is that now that the issue is in the spotlight, the government may enforce the law, but what happens when the noise dies down? “Who would buy the far more expensive syringes when they could make do with the cheaper option?” He questioned, adding that the wholesalers would eventually lose out on their investment.
What now
Back at the Rato Dero Taluka Hospital, the worried mothers waiting in line for hours to get their children tested, would beg to differ. R*, who had brought her four children, looked like she was close to a nervous breakdown.
Three of her children had been treated by Dr Ghangaro. As soon as she had heard of the outbreak from a lady health worker, she had taken a rickshaw from her village, Sajjan Makray, a half hour away, to come to the facility.
Several hours later, she was relieved to know that none of her children had been affected. At least 558 others have not been so lucky.
The victims will now undergo therapy for the rest of their lives. “HIV patients receive a dose of the ART medication every month,” said Soomro. The medication is expensive, with each patient incurring a cost of Rs30,000 per month. Then there is the availability issue. The medicine is imported from India by the WHO, which then hands it over to the provincial health department.
For now, the Global Fund is assisting the provincial government cover the cost of the treatment and pledges to do so for the remainder of the patients’ lives. “This is a huge cost on the already burdened health department,” noted one district-level health department official, asking not to be named. “If the SHCC, SACP and other monitoring agencies had just done their job, we wouldn’t have had to deal with this,” he remarked.
Even the drug abusers in Larkana seem to understand this much. “We don’t welcome those using syringes here,” said one addict, who was huddled with a group of six men smoking crack heroin under a flyover in Larkana. “We have heard about the epidemic and don’t want them causing problems here, so we shooed them away,” he said.
When the provincial government and its health agencies will finally rise to the challenge remains to be seen. “Hopefully this time, whatever action or policy they make will have a lasting effect,” said the health department official, referring to the previous outbreaks when the authorities’ will to effect change died out with the interest of the news channels.
For the children and their parents, however, life will always revolve around that fateful prick of the needle. For most, that reality hasn’t really sunk in yet. One middle-aged man who had brought his one-and-a-half-year-old daughter to the Children’s Hospital, didn’t know anything about the disease. “The doctors haven’t really told me much,” he said nonchalantly. Like so many others, his daughter too had tested positive for the virus at the Rato Dero Taluka Hospital and had been referred to the facility. “But I believe she will be fine,” he added. “InshaAllah.”
LATEST






MOST READ

Pak pilgrims slam Hajj arrangements

Industrial estate approved along Rawalpindi Ring Road

Twin cities witness sluggish trade activity

Pakistan plans oil reserves, storage push as Hormuz constraints expose vulnerabilities

Pak-China friendship will grow broader like Karakoram Highway






COMMENTS
Comments are moderated and generally will be posted if they are on-topic and not abusive.
For more information, please see our Comments FAQ