
As of February 19, 2021, according to the Covid-19 Health Advisory Platform by the Ministry of National Health Services Regulations and Coordination, Pakistan had 568,506 confirmed cases of cornavrius, and 12,527 total deaths since the pandemic first arrived in the country. In the 24 hours preceding February 19th, 1,245 new cases and 40 deaths were recorded. A total of 531,840 positive Covid-19 cases have recovered and about 1,626 cases are in critical condition as of the time of writing this article. So far, 8,602,515 tests have been conducted across the country and our daily testing capacity has hovered around the 35,000 mark since September 2020; out of a total available capacity of 59,98. Before that, it was hardly around 20,000 tests a day. Pakistan’s daily death count attributed to Covid-19 has been quite stable, around 50; however, it once climbed as high as 124 on June 15, 2020, and 111 on December 23, 2020. In June 2020, Pakistan’s positivity rate had reached about 9%, but ever since then it has been on the decline, and currently it stands at less than 4%.
So does this data suggest that Pakistan has managed to limit the impact of the pandemic, and, if so, does that imply that countries like Pakistan have been shielded from the full-blown ramifications of Covid-19 compared to countries like Spain, Italy or England? The proponents of this assumption reason that the caseload of Covid-19 and the mortality rate has been comparatively low in Pakistan despite the fact that few people have followed the Standard Operating Procedures (SOPs). We know that most people in Pakistan cannot afford social distancing measures since they use public transport and work in closed environments. Buying soaps, masks, and hand sanitisers may also be challenging for most people with a low monthly income. Given this, and the fact that many people believe in conspiracy theories surrounding the pandemic, the odds of the masses as a whole following the SOPs, as advised by the government, are extremely low. Therefore, this behaviour increases the risk of virus transmission within and across communities. This begs the question as to why, despite this elevated level of exposure to the virus, has the case and death load as a result Covid-19 been relatively low in comparison to more economically developed countries? The answer to this question is not easy as it seems because we lack adequate research on Covid-19 from Pakistan, but a logical analysis based on the existing knowledge about the pandemic may give us some answers.
To me the impression that we have been somehow spared by the pandemic is simply false. Why? Let us first have a look at the age structure of Pakistan before answering this question, because age has a lot to do with the severity of a Covid-19 infection and its Case Fatality Rate (defined as the percentage of deaths from the positive cases). Pakistan’s population has a higher percentage of young people as compared to its older population. This is because of a high fertility rate adding up to the pool of the young population, and a poor survival rate at an older age because of chronic diseases, but mainly from poor access to quality healthcare services. Currently, the median age, the age which half of the population is under and the other half is over, is 22 years. The population in the age group from 55 to 64 years is 5.55%, and 65 years and over is only 4.4%. Because we know that both the mortality rate and mortality risk from Covid-19 increases with age, our population may not be simply at elevated risk of deaths. Therefore, elderly persons have a higher risk of dying as shown by the data from countries like China or Italy (see Figures 1 and 2), where the mortality rate among patients with Covid-19 infection above 80 years of age has been shown to be 14% compared with only 1.3% in patients between the age of 51 and 59 years. We also know that the average life expectancy in Pakistan is around 65 years, compared to more than 80 years in most high-income countries, and people from low-income groups in Pakistan do not even survive beyond the average life expectancy of the country. This, and the fact that economically well-off elderly individuals in poor countries can afford to be protected from Covid-19 infections, ensures that relatively fewer elderly persons are dying of Covid-19 in Pakistan (Figure 3) in comparison to the statistics from other countries. There are simply not enough elderly people in the population who are exposed to the virus. The virus could be multiplying amongst the younger population since within this group the infection often occurs without any symptoms.
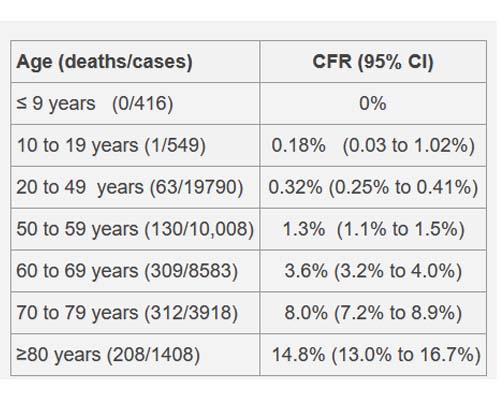
Figure 1. Actual Case Fatality Rate by age (%) in China, March 2020, Source: The Centre for Evidence-Based Medicine
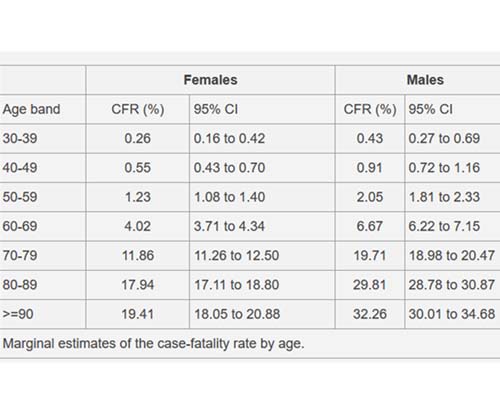
Figure 2. Estimated Case Fatality Rate by age (%) in Italy, March 2020, Source: The Centre for Evidence-Based Medicine
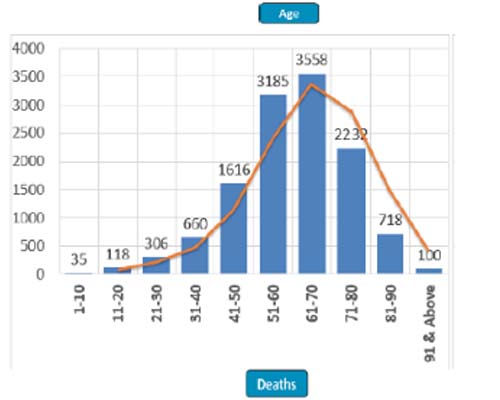
Figure 3. Age wise Covid-19 related mortality in Pakistan. Source: National Command And Operations Centre Situation report
But why are more patients with Diabetes Mellitus or cardiovascular diseases in Pakistan not falling prey to complications as a result of Covid-19, even though 17% of Pakistan’s population has Diabetes? The risk of Diabetes in Pakistan starts at much younger age compared to in the west. In a recent study of 18,856 persons, 16.1 persons between the age of 20 and 30 years either had pre-diabetes (impaired blood glucose levels but not high enough to diagnose as Diabetes) or Diabetes Mellitus. This shows that a large majority of the patients with Diabetes Mellitus in Pakistan are younger than their western counterparts. Therefore, a younger age of the persons with Comorbidities could be the reason that more of these patients may be protected against severe Covid-19 infections or its complications. Diabetes Mellitus increases the risk of requirement for critical care and mortality as one Scottish study notes, but this study, which had 90 % Diabetics above the age of 60 years who were admitted to critical care after a Covid-19 infection, also supports the proposition that young Diabetics could be protected against severe illness and death in Pakistan; and even if they develop severe symptoms, they may attain full recovery, thereby attenuating our daily count of Covid-19 related deaths.
Another issue is of the availability of quality data: the elderly and patients with Diabetes could still be dying because of Covid-19 but since case detection and contact tracing in Pakistan is not adequate, both cases and deaths could be hugely underestimated. With about 35 tests per 1000 individuals, Pakistan’s testing capacity has been dismal compared to other countries. While it is understandable that we cannot compare Pakistan with more economically developed countries like America, where about 945 tests per 1000 individuals have been conducted so far, or the UAE, where testing capacity so far has been three times that of the population size, poor testing could be a reason for our lower detection of the actual burden of Covid-19 in Pakistan. If we had a testing capacity comparable to that of the countries in the Figure 4, we may have ended up counting more cases; and for that reason, we could have recorded more deaths from Covid-19 in the communities for which a cause of death is not currently ascertained. Since a reliable system for registration of births and deaths is not present in Pakistan, it gives further strength to this speculation that there could have been more deaths in Pakistan due to Covid-19 than are currently being reported.
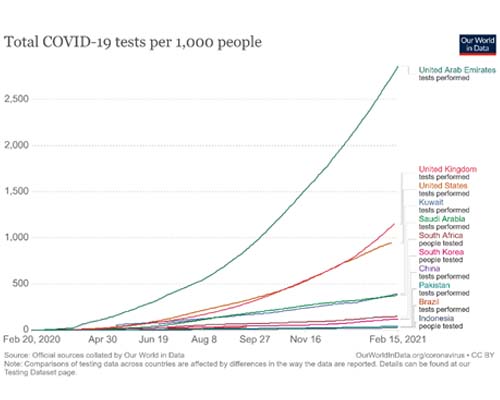
Figure 4. Covid-19 testing capacity per 1000 selected countries.
And this notion of calling Pakistan’s risk of Covid-19 “low” and comparing it with the rest of the world is based upon a basic fallacy. So how “low” is this risk of mortality from Covid-19 in Pakistan? With only about 10% of the population over the age of 55 years, the daily death count of 40 is not insignificant. Many of these middle-aged people who are sick and elderly continue to work for an earning in Pakistan for their families, and most, unlike in the welfare states of Europe, have little or no support from the government to sustain a reasonable quality of life. Therefore, by losing these 40 people to Covid-19 a day, we are still losing people who by the definition of elderly may not be that elderly as they are considered in the west. Agreeing with the fatalists who believe that these elderly persons have lived far beyond their expected life span is a fallacy. Also, as stated before, our life expectancy of 65 years is already about 20 years lower than the populations in the west, where the longevity continues to improve far beyond 90 years and the presence of octogenarians in these populations is not surprising these days, thanks to high-quality healthcare, healthy lifestyle, and healthy living conditions.
If we factor in the low intensive care unit bed occupancy rates in Pakistan into the equation to explain low mortality rate from Covid-19 in Pakistan, the 2,942 Covid-19 isolation beds available throughout the country must have been sufficient and very well-equipped with trained staff catering to the needs of patients with the illness requiring no intensive care, because the patients with mild illness were receiving treatment in their homes. These hospital beds never became overwhelmed except during the second wave of the pandemic in the winter of 2020, when the bed occupancy rate touched about 95%. The daily case load reported at that time touched about 3000 before dropping to half of that in January 2021.
Currently, as of February 19, 2021, 241 patients are in the intensive care units throughout the country requiring ventilator support for breathing (Figure 5). The data from the National Command and Operations Centre shows that in most cities, like in Lahore, the ventilator occupancy rate currently is as high as 36%. All this evidence points towards the reality that our healthcare system, although not well prepared in advance when the pandemic started, has still been able to deal with the existing burden of the critical cases, ensuring fast recoveries in most patients with mild to moderate illness, but has not been able to prevent deaths among older persons and those with a coexisting illness like Diabetes Mellitus, high blood pressure or obesity.
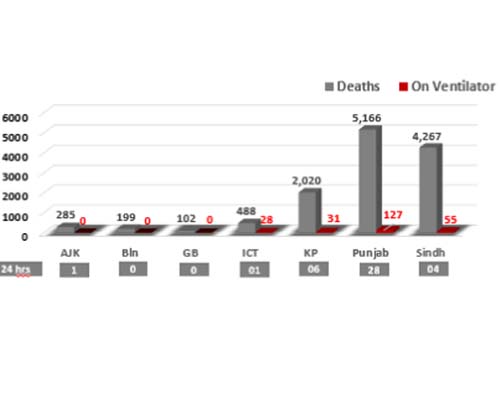
Figure 5. Province wise tally of deaths, and critical patients due to Covid-19 in Pakistan. Source: National Command and Operations Centre Situation report
Therefore, our part of the Covid-19 pandemic also calls for similar attention and intervention as it does in the west. The younger population needs to continue to protect the elderly and persons living with comorbidities like Diabetes Mellitus and high blood pressure; they must take special precautions to avoid transmitting the virus to the elderly in their families. This may not be easy as the love and bonding between generations is deeply entrenched in our culture and the blessing of having an older parent and/or a grandparent in a home is highly valued and cherished. However, close contact between asymptomatic young people and unvaccinated older persons can lead to severe infections in the later. This is the reason people were prohibited from seeing their elderly parents and grandparents in care homes across the UK because the morality rate among the elderly almost doubled during the pandemic. Although these measures were drastic and had negative impacts on the mental wellbeing of the elderly and their children, they were necessary to extinguish the raging flames of the pandemic in care homes. What we can do is create awareness among the population to limit close contact with the elderly, especially when the young ones have any of the Covid-19 related symptom or exposure to a recently confirmed case of Covid-19. Encounters in unventilated and closed spaces must be avoided and limited to less than 15 minutes and masks need to be worn at all times when meeting or coming in contact with the elderly, especially frail, sick, and vulnerable persons.
The long-term solution to our way out of the pandemic would be to achieve herd immunity where about 70% of our population develops immunity to the virus. This is not possible in the near future, as our community seroprevalence rate is only about 15% and vaccination has not yet begun for the general population. So what can be done in these circumstances? About 20 million people above the age of 51 years of age in Pakistan need to be considered as our priority to prevent infection in; then, as more vaccines become available, we must vaccinate the younger populations (remember that the young are considered super-spreaders of the infection as they can harbour the SARS-COV 2 without any symptoms at all). The best way to achieve this is to vaccinate the older population without any further delay. This could be a challenging task considering the lack of resources. The delivery of 17 million doses of vaccines to Pakistan through the COVAX initiative is expected in April, but this may not be enough as this will only protect for 8.5 million people in Pakistan (most vaccines require two doses) and that will also include healthcare personnel, which should be our top priority. Steps need to be taken to obtain adequate doses of vaccines and set up a fast in-country storage and delivery system so as to make the vaccine available and accessible to the older populations in vulnerable communities. How the rural populations, who are at higher risk of Covid-19 infection because of their limited access to vaccine knowledge and awareness, will be vaccinated also needs to be considered. The recent announcement that the private sector will be authorised to obtain vaccines is a welcome initiative, but the poor may not deem it necessary to buy a vaccine out of their own income because, according to the announcement, the private sector will be exempt from any price limits by the government and prices could be out of the reach of the poor.
COMMENTS
Comments are moderated and generally will be posted if they are on-topic and not abusive.
For more information, please see our Comments FAQ