Farida Bibi lived near Lower Dir, in Shahi Bin Shahi, a remote area of the Khyber Pakhtunkhwa (KP). Last year in December, she developed serious labour complications. Since the local basic health unit did not have facilities to treat pregnant women, a lady health worker advised her husband to shift her to Peshawar. “Her condition is critical,” she told Javeed Khan, Farida’s husband, who rushed to call an ambulance.
A dilapidated road connects Farida’s village to the town of Lower Dir, from which, Peshawar lies at a distance of at least six hours by road. After the devastating monsoon floods last year, the condition of roads in the periphery, which was far from, sound to begin with, had further deteriorated. When the ambulance finally reached Farida, her condition had worsened. “It is unfortunate that in this day and age, we still lack basic health facilities or doctors to treat expectant mothers going through the ordeal of childbirth,” said Khan.
Drowned infrastructure
According to a 2019 maternal mortality survey, 186 women died for every 100,000 births and 11,000 maternal deaths occurred each year in Pakistan, which has the highest fertility rate in South Asia.
In northwestern KP where Lower Dir is situated, the fertility rate is higher than the national average. The annual growth rate of population in KP is 2.89% (1998 to 2017), according to the Pakistan Demographic Health Survey (PDHS), while the annual maternal deaths are 1900. Out of 1000 live births, 53 infants die in the first year of birth, and 23% per cent of children under five years of age are malnourished and underweight.
Throughout the journey from her village, Farida cried for help while her husband tried his best to calm her down. As the road was bumpy and the distance long, Farida soon became unconscious. “She had internal bleeding, and looked at our two little daughters as if she was asking for help,” says Khan, adding that the recent flood had washed off the roads, leaving entire villages stranded. He kept asking the ambulance driver to go faster but the roads were hard to traverse and their journey was far from smooth.
The countrywide floods that affected 31million people have destroyed the basic infrastructure in villages and towns in the periphery. According to a report by the Population Council of Pakistan (PCP), 18 million people were affected in 16 districts of Sindh, 4.8 million people in Balochistan, 5.7 million people in Punjab and 2.3 million people in KP.
The PCP report shows that out of 0.6 million currently pregnant women in Pakistan, 380,000 live in the severely affected districts in rural Sindh, 77,000 in Balochistan, 110,000 in Punjab and 43,000 in the flood-affected districts of KP. Around 93,000 women in KP live with unmet health needs in the severely affected districts, 386,000 five year-old children require immunisation, and 43000 currently pregnant women need antenatal and postnatal delivery services.
The floods have badly affected women’s health, especially pregnant women. In KP, the worst affected among districts is Dera Ismail Khan where 22,849 pregnant women were affected, 6833 in Chitral, 13,596 in Tank, 46833 in Mardan, 33,135 in Swat, 29020 in Swabi, 53,870 in Peshawar, 9075 in Kohat, 24215 in Mansehra, 33131 in Bannu, 33005 in Bajaur, 20532 in Buner, 36003 in Nowshera, and 30,084 in Charsadda.
The report further shows that 93000 women in severely affected districts expressed a desire to space or limit their children, but remain unserved, and 121,000 women in severely affected districts bear five or more children.
The three Ds leading to death
Pakistan’s huge population of 207.8 million is growing faster than most regional and Muslim countries. Between the last two censuses of 1998 and 2017, the country’s population grew at 204% per year. It is projected to reach 285 million by 2030, and that estimate may double in the next 30 years.
Fertility in Pakistan, at 3.6 average births per women, is twice the level of Iran and higher than Saudi Arabia (both Muslim countries). A large number of couples in Pakistan want to space or limit births, but are unable to do so due to lack of information or services. According to the PDHS survey, unmet needs for family planning service is high at 17%.
The main barriers to contraceptive use include physical distance from delivery points, cost, social barriers, and poor quality of service and associated misconceptions. Millions of desperate women resort to induced abortion every year, often in unsafe conditions that compound maternal and child health outcomes. Poor and uneducated households are most affected and poverty in the country is closely related with low literacy, high fertility, and high childhood and maternal mortality.
When there is low public expenditure on health, population and education, it is visible through poor socio-economic development. In Pakistan, nine million pregnancies occur per year, with four million of them being unwanted. Annually, the number of induced abortion is 2.2 million, with 1.4 million unwanted births and 0.4 million miscarriages.
Under a judicial order, a national and provincial task force was established to reduce population growth through family planning and increased contraceptive prevalence rate, but the provincial and federal government representatives seem to have a non-serious attitude. Citing figures from the PPC and PDHS reports, Dr Khizer Hayat, Director Maternal Child Health, says that in KP, 165 children per 100,000 live births die every year.
“In KP, primary, secondary and tertiary health care facilities are available for patients, with an upgraded 200 basic health units across the province,” he says. “But the 3Ds ― delay in reaching care, delay in seeking care and delay in receiving care ― cause deaths of mothers and children. An expectant mother should at least make four antenatal care visits to the hospital.”
Dr Hayat pointed out that in the flood-affected areas of KP, particularly Charsadda, Nowshera, Swat, Peshawar, Tank and other districts, health authorities were providing medicine and gynaecological care through free medical camps to pregnant women. In addition, 16,500 lady health visitors go door to door to create health awareness among women. “We request couples to keep the size of their families at a minimum and involve women in family planning decisions.”
Girls and brides
After August 2021, following the Taliban takeover in Kabul, Nazakat Bibi fled Afghanistan and now lives with four siblings in Peshawar. Her husband works in a local hotel as a waiter.
“I have two daughters and two sons, and I am pregnant again since the last eight months, with no money to see a doctor,” she says. Nazakat’s family were compelled to migrate from Afghanistan and leave their home behind because the Taliban did not allow girls’ education, and it was her dream to educate her daughters.
According to a UN High Commission for Refugees report, Pakistan currently hosts 1.3 million documented and almost as many undocumented Afghan refugees. Of them, the majority resides in the northwestern KP, which serves as a gateway to Afghanistan.
The report shows that after the recent Taliban takeover in Afghanistan, around 250,000 Afghans came to Pakistan. Most of the refugees settled in Peshawar, with women and children suffering complex health issues.
With one woman dying every two hours due to preventable pregnancy and childbirth complications, Afghanistan has the highest maternal death rates in the Asia and Pacific region. Women’s inaccessibility to facilities for safe deliveries is one of the contributing factors to this grim situation.
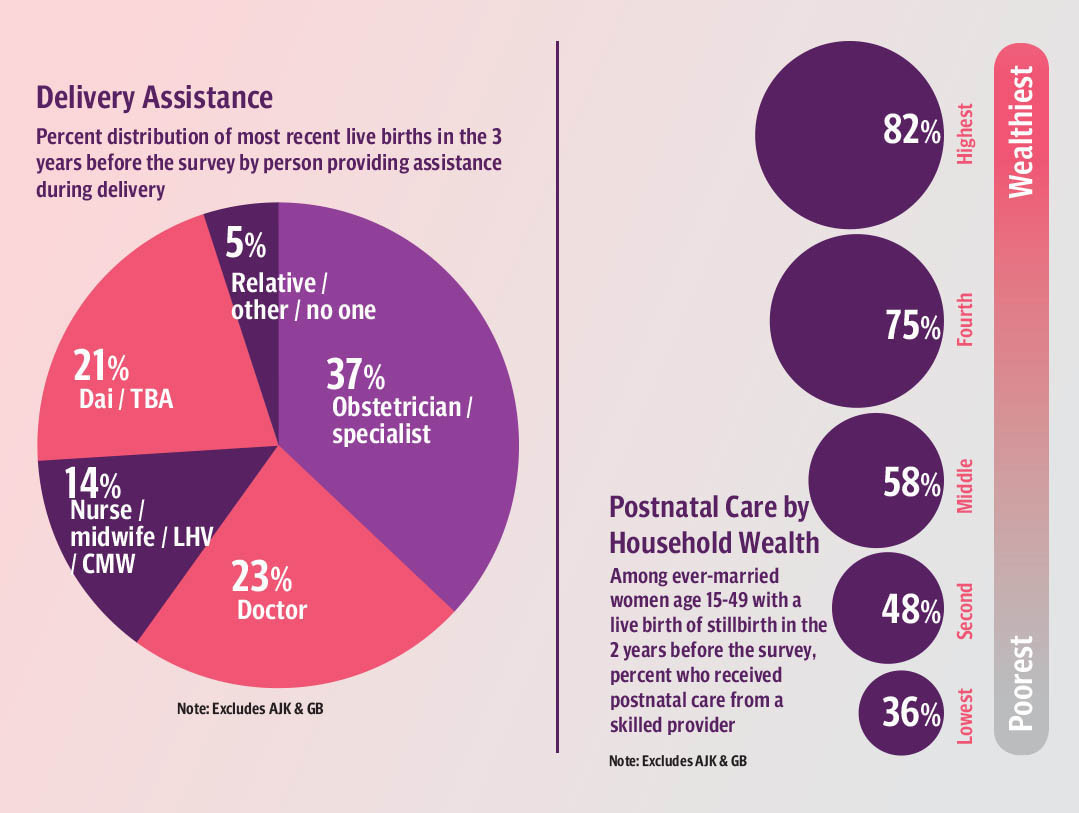
According to the United Nations Population Fund, in Afghanistan a skilled healthcare worker attends only 14% of births with most of the pre- and post-natal care provided by a midwife, instead of an obstetrician.
According to Girls Not Brides, a global network committed to ending child marriages, 28% girls in Afghanistan are married before the age of 18, 4% before their 15th birthday, 7% Afghan boys are married before they are 18, and 522,000 women are married or in a union before the age of 18, which ranks 20th highest in the world.
According to the UN women report, Pakistan has the 6th highest number of girls married before the age of 18. A World Bank study from 2017 says child marriage will cost developing countries trillions of dollars by 2030.
According to Sana Ahmad, a KP-based social worker and Human Rights activist working for women rights, child marriages increased in KP due to the pandemic and ensuing financial problems of the parents who wanted to marry off their daughters as soon as possible so they don’t have another mouth to feed.
“Due to lack of awareness and cultural barriers, mostly girls below 18 were married,” says Ahmad. “When a girl is married off at 14 or 16, she and her newborn suffer health complications. In the rural areas of KP including Dir, Swat, Chitral, Kohat, Hangu, Charsadda, Kurram Agency and other merged areas, child marriages are rampant as there is no implementation of law, despite the government passing several bills and laws.”
Samia Ali Shah, project director of PCP, says that the authorities have never properly addressed women’s health issues or taken the population control task force meeting seriously. “In all provinces of Pakistan, the meeting is to be held by the chief ministers, but so far it has not been a priority for them.”
According to the PDHS report 2017-18, Shah says, the percentage of married women of reproductive age who expressed a desire to either prevent or delay child birth was 15.5%, however, only 34.2% use contraception
“In rural KP, contraceptives for family planning are not available in stores because of social taboos and even if they are available, men can’t buy them openly,” she says. “Also because of the pandemic and the recent floods, the economic situation of people is so bad that they cannot really afford contraceptives.”
Dr Farooq Jameel, special advisor to the chief minister on health says that the population of KP has been increasing at an alarming pace and although the prices of contraceptives had hiked due to the pandemic, the provincial government had provided them to all family planning centres in the province.
According to Dr Jameel, the government was committed to control the rapid increase of population. More than 36 family planning centres were established across KP including merged areas of FATA and more were being planned across the province as well as in merged areas of KP.
The provincial government has also constituted a provincial population task force under the chairmanship of the chief minister for population control through various government and the private sector programmes. The task force has approved a five-year action plan as well as a provincial narrative on population welfare.
Yet, conditions on ground are grave when it comes to mother and child healthcare. Dr Fatima Ali, a gynecologist at Lady Reading Hospital, Peshawar, says that when women in labour come from areas such as Chitral, Upper Dir, Kohistan and other fur flung areas of Peshawar, by the time they reach the hospital, they are mostly struggling for life because of poor road conditions and long distances.
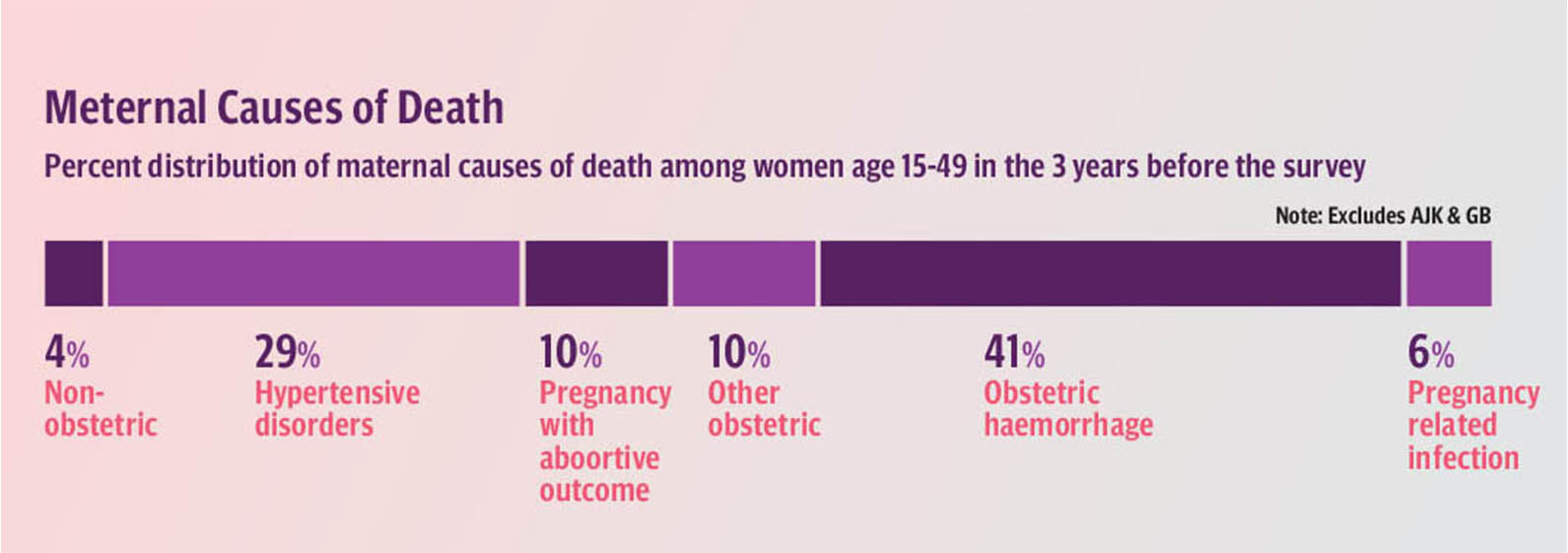
“Clerics should give speeches in mosques and other cultural places like hujras to take care of pregnant women and get them checked by doctors regularly,” says Dr Ali, emphasising on print and electronic campaigns to create mother and child health awareness. “Lady health workers are not trained for childbirth and women prefer to give birth at home because of social taboos which is dangerous for the mother and child. Since most pregnant women are anaemic, internal hemorrhages and blood loss are major causes of death among pregnant women.”
This was what had happened to Farida, who was internally bleeding in the ambulance and breathed her last on her way to Peshawar. She and her family had prepared for the baby’s arrival but not for her pregnancy and complications.
A broken Khan had told the driver to turn back home as his wife Farida was no more.
“If steps are not taken now, maternal deaths will continue to happen,” he says. “Basic health units and other facilities in the area must be upgraded, the budget for maternal and child healthcare increased and all possible facilities should be provided to people at their doorsteps. When you lose a mother, you lose an entire generation.”